

A hospital pays a travel nurse agency a bill rate for every hour worked. The nurse typically receives somewhere between 55 – 70% of that rate, while the rest covers the agency’s overhead, benefits, and profit margin, which is usually 20 – 45% of the bill rate depending on how it’s calculated.
Some estimates for total markup run even higher, up to 65%, when agency-specific costs and negotiation leverage are factored in.
For a hospital running dozens of travel contracts at once, that spread adds up fast. It becomes the line item a CFO questions at every board meeting, a cost that stands out from the rest of the budget.
If you’re looking for ways to cut travel nurse costs, you’ve come to the right place. In this blog we’ll share seven alternatives to travel nursing agencies for hospitals.
Why Hospitals Are Moving Away from Traditional Agencies
The markup is only part of the problem. Most finance teams struggle to get a clear breakdown of how it’s calculated, which makes it hard to challenge. Three other issues compound this:
- The relationship ends with the contract. A nurse who performs well for 13 weeks goes back into the agency’s pool, not the hospital’s. If that unit needs help again in six months, there’s no guarantee the same nurse comes back.
- Quality depends entirely on the agency’s vetting. Standards vary from vendor to vendor, and the hospital absorbs that risk when a placement doesn’t work out.
- Most hospitals rely on just 2 to 3 vendors. That concentration leaves little leverage when a vendor raises rates or can’t fill a request in time.
None of this means agencies disappear from the picture. It means more hospitals are running multiple sourcing channels at once instead of depending on one.
7 Alternatives to Travel Nurse Agencies
The following are 7 alternatives hospitals can pursue if they want to get the middleman out while retaining the ability to source qualified talent.
Private Talent Marketplace
What it is: A Private Talent Marketplace is a hospital’s own branded, AI-powered hiring platform. One that pulls together every source of talent the organization already has access to but isn’t fully using, alongside newly sourced contingent talent, in one place.
That means current employees open to internal mobility, past applicants sitting dormant in the ATS, alumni who’ve worked with the system before and new contingent talent. All of it lives in one place, matched by verified skills instead of keyword-searched resumes.
SkillGigs’ Private Talent Marketplace works this way. Instead of calling an agency every time a unit needs coverage, the hospital can search its own talent marketplace first, drawing on the people it already knows along with newly sourced contingent talent and fill the position from there.
Best for: Health systems with meaningful hiring history, an existing workforce, or a mix of both, that want to manage internal and contingent talent under one roof and build a talent pool they own over time.
Tradeoff: Setting up and activating a private marketplace takes some initial work. Data has to be integrated, skills mapped and the platform linked to existing HR systems. For systems trying to break free of agency dependency, it’s the right choice
Internal Float Pools / Internal Travel Programs
What it is: A hospital that sees the need for additional help goes to staff from within units or facilities to move around in an internal float pool. Some systems structure this as an “internal travel” program, meaning the staff nurse receives a travel contract and an increase in salary to fill in shifts at a sister facility.
Best for: Multi-facility health systems with cross-trained staff.
Tradeoff: It will only work if you have more than one facility or nurses who are credentialed to float between facilities. This is not possible with a one-site hospital.
Direct-Sourcing Marketplaces
What it is: These platforms connect hospitals directly with clinicians, removing the agency from the middle of the transaction. Many platforms work this way. The hospital sources, reviews, and contracts the nurse directly. The ongoing workforce management that an agency would normally handle shifts to a dedicated service like CTM.
Verification is what makes this model viable at scale. Tools like SkillsCreed handle the vetting an agency would otherwise do, credential checks, competency validation, and work history review.
Skip this step, and direct sourcing just swaps agency markup for agency-level risk without the agency’s screening. That tradeoff gets overlooked in most conversations about this option.
Best for: Hospitals with enough hiring volume to justify running their own sourcing pipeline, or systems planning to reduce agency reliance over the next year or two.
Tradeoff: Even with verification tools in place, some sourcing and screening work shifts onto the hospital’s own team. It’s a cheaper model, but it isn’t a hands-off one.
On-Demand / Per Diem Staffing Apps
What it is: Apps that fill local, shift-by-shift gaps. Consider it as a nurse taking one 12-hour shift near you, not a 13-week contract. The platforms have a competition of speed and flexibility, rather than long-term coverage.
Best for: Short-notice, single-shift gaps especially in cities or suburbs with a deep local nurse pool.
Tradeoff: These apps solve for right now, not continuity. They work well alongside a bigger sourcing strategy, but they can’t cover a long-term vacancy or a specialty unit on their own.
Managed Service Providers (MSPs)
What it is: An MSP will handle your interactions with several staffing companies. It brings vendors together, streamlines rates, manages compliance and invoicing. That’s a significant cut in administration time!
However, an MSP doesn’t eliminate the agency layer. The nurse is still not contracted directly with the hospital. The MSP just sits between the hospital and a network of agencies, which still sit between the hospital and the nurse. It still has a lot of markup, but it’s just been handled better.
Best for: Large systems with many departments and high contract labor volume, where vendor consolidation is more important than a total reduction in mark-up.
Tradeoff: Less admin work, but the agency economics don’t go away. They just get organized.
Reactivating Your Own ATS Data
What it is: The option most hospitals already have and don’t use. When someone is applying to a hospital job, their credentials are often either pre-screened or have been interviewed years ago and are just sitting in some hospital’s applicant tracking system.
That’s a pool of pre-vetted candidates that most hospitals never look at again because a nurse applied a long time ago, made it through the phone screen and was not hired for some reason that has nothing to do with the nurse’s qualifications.
That pool is put to life automatically when tools are created to activate ATS data. Transforming an archive into a live source channel.
Best for: Hospitals that have an ATS for a few years and have some volume of applicants to work with. That’s most hospitals.
Tradeoff: Data quality matters here. If old applicant records are incomplete, you’ll need to clean them up before this is useful.
Regional Hospital Alliances / Staffing Consortiums
What it is: It is a regional pool of contract labor from multiple health systems. They sometimes negotiate as a group with the agencies. They sometimes create a common internal float pool in organizations.
Best for: Regions with several systems facing similar seasonal or specialty gaps, where negotiating power outweighs the coordination work.
Tradeoff: This needs ongoing cooperation between organizations that are often competing for the same patients and staff. This restricts its scaling ability.
How to Choose the Right Alternative for Your Hospital
These choices typically boil down to two considerations that CFOs and CNOs must balance which are control over cost and speed of replacement without disruption to continuity of care.
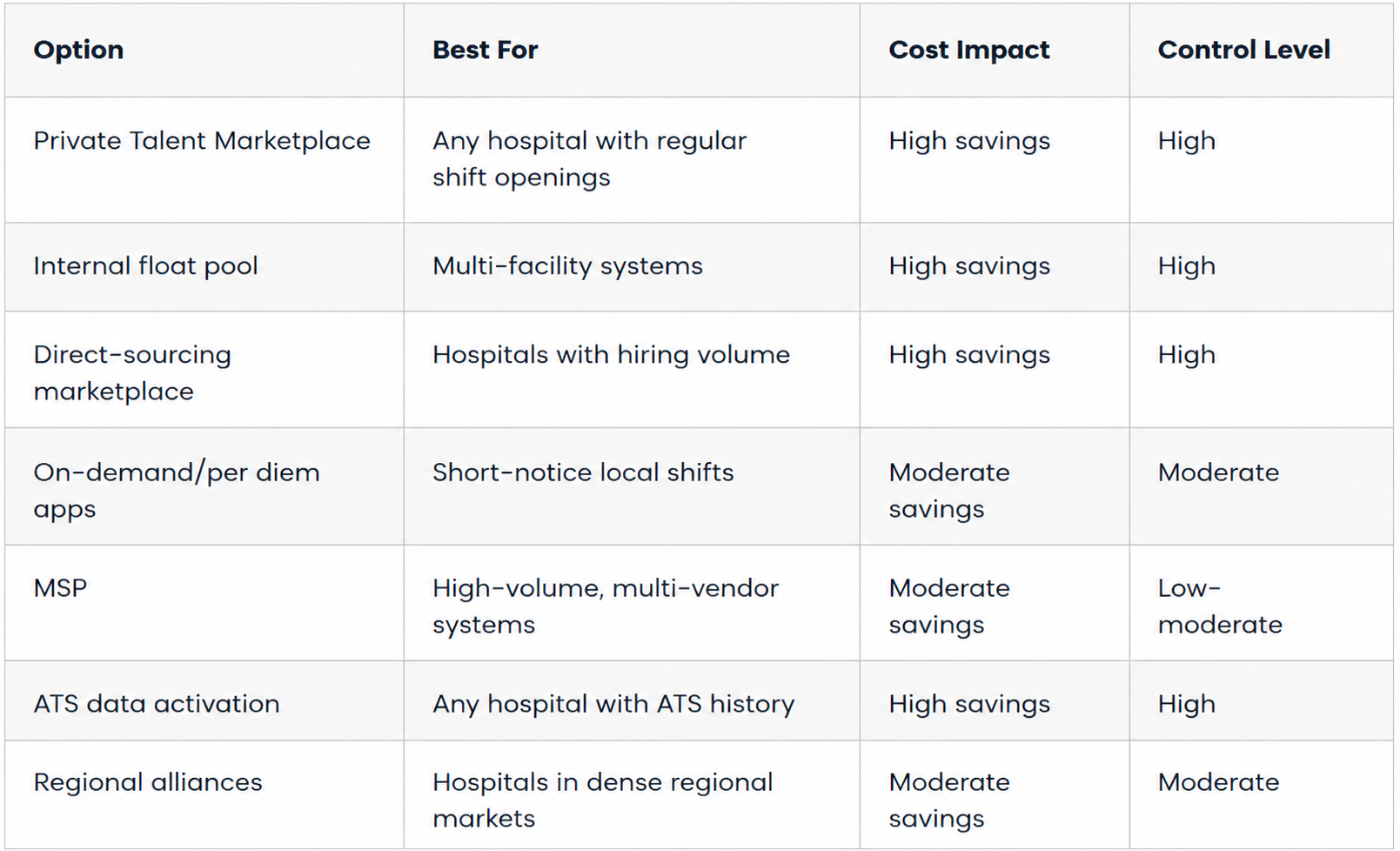
If you’re chasing an urgent, single-shift gap, per diem apps make the most sense. If you’re trying to cut contract labor spend for good combine direct sourcing, ATS reactivation and internal float pools. Those three hand the most control back to the hospital.
What Hospitals Gain by Cutting Out the Agency Layer
The clearest way to see the value is to look at what actually changes day to day, not just what you save on paper.
The first change is rate transparency. A hospital that sources a nurse directly sees the actual rate paid to the nurse, not a bundled bill rate with markup folded in. Finance can plan around a real number instead of guessing at one.
The second is ownership of the relationship. Once a contract ends, a directly sourced nurse stays in the hospital’s own pipeline. She doesn’t disappear into an agency’s files until the next opening comes up.
The third is verification replacing the vetting an agency used to handle. Skills verification tools confirm licensure, competencies, and work history the same way an agency would, minus the markup for doing it.
This isn’t a niche shift. SIA research shows 60 percent of enterprise buyers are already exploring direct sourcing as a strategic priority, and that number is expected to climb over the next two years.
The hospitals moving on this now are the ones setting the terms. The ones waiting are negotiating from a weaker position with every contract cycle that passes.
FAQ Section
Are direct-sourcing nurse platforms cheaper than travel nurse agencies?
Usually, yes. Direct sourcing removes the agency’s markup which is typically 40% to 60% of the bill rate. That means a lower cost per contract in most cases. The tradeoff is that the hospital takes on more of the sourcing and screening work itself.
What is the average markup on travel nurse agencies?
Markups usually fall between 40% and 60% of the bill rate a hospital pays. This will vary according to specialty, contract duration and location.
What is an MSP (managed service provider) in healthcare staffing?
An MSP will oversee your hospital’s dealings with multiple staffing agencies. It unifies vendors, simplifies compliance and manages invoicing. It saves administration time but does not eliminate the agency between the nurse and hospital.
What is the difference between an MSP and a direct-sourcing platform?
An MSP organizes and manages agencies you’re already working with. You’re still contracting through them. A direct-sourcing platform skips that step entirely. The hospital sources, vets and contracts with the nurse directly.


